Construction is one of the most dangerous industries for cardiac events in the United States — a function of older workforce demographics, heat stress, exertion, electrical hazards, and EMS response times that can exceed 15 minutes on remote sites. The NIOSH notes construction workers experience disproportionately high cardiovascular event rates compared to general industry, particularly for workers 45+.
This guide walks general contractors, safety officers, and project managers through OSHA-aligned AED placement on construction sites — from a small residential remodel to a 50-story commercial high-rise. Every recommendation aligns with OSHA 1926 (Safety Standards for the Construction Industry) and current AHA guidance.
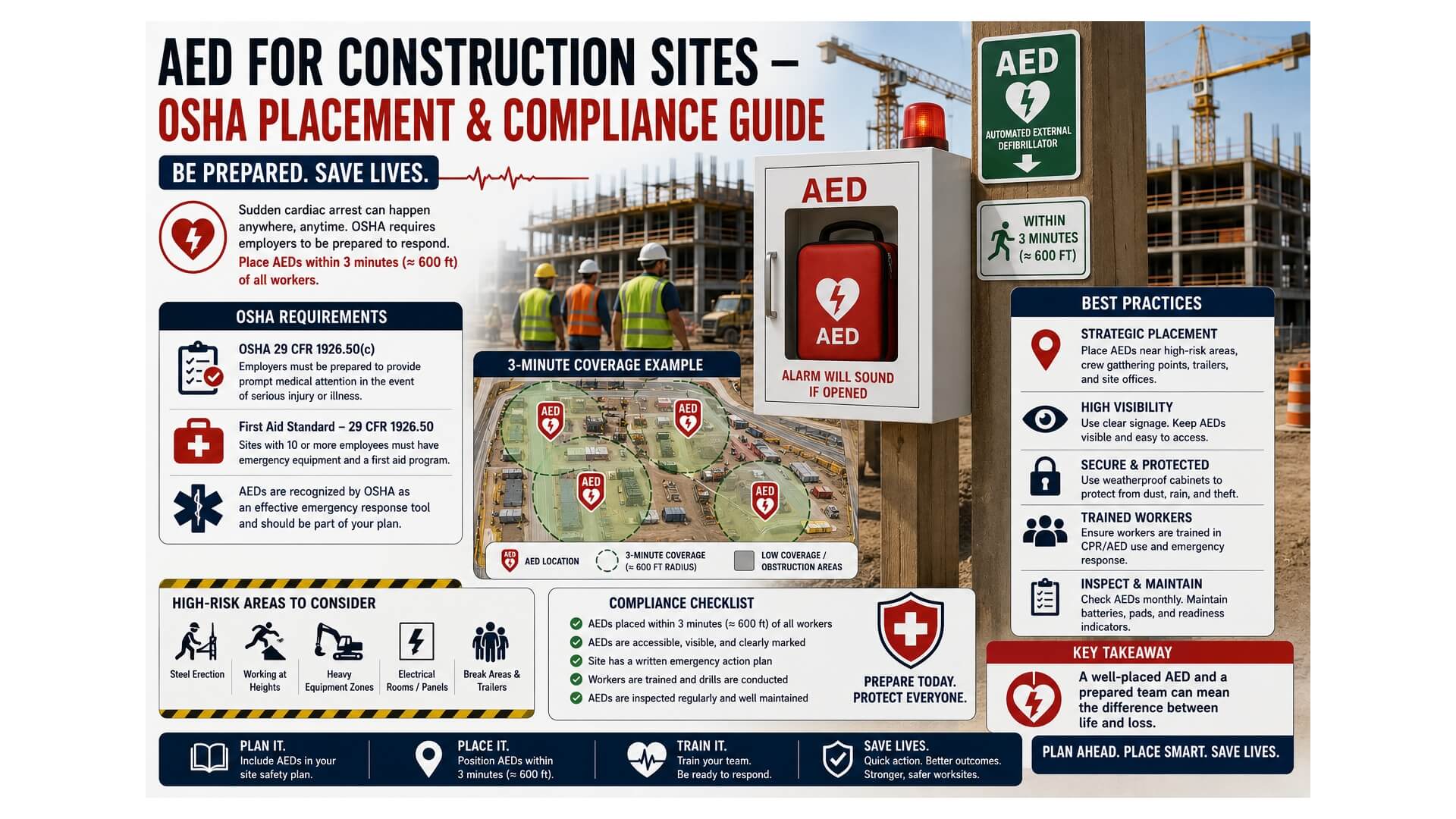
The OSHA position on construction-site AEDs
OSHA 1926 (the construction-specific safety standard) does not mandate AEDs on jobsites — but the OSHA Best Practices Guide recommends them at any site where:
- EMS response time exceeds 5 minutes
- 50+ workers are on-site simultaneously
- The work involves elevated cardiac risk (heavy exertion, heat stress, electrical work)
The OSHA General Duty Clause (29 USC §654 5(a)(1)) makes the legal argument stronger: cardiac arrest on a construction site is a foreseeable hazard, and not providing reasonable response capability creates legal exposure for the GC and the site owner.
Coverage math for construction sites
Construction sites are unlike any other facility — they’re temporary, change shape daily, and combine outdoor exposure with confined indoor work. The placement math becomes:
| Site type | Minimum AED count | Placement strategy |
|---|---|---|
| Residential remodel (1–10 workers) | 1 | In the jobsite supervisor’s vehicle or the onsite tool crib |
| Single-family new construction (10–25 workers) | 1 | Foreman trailer or site office |
| Mid-size commercial (25–75 workers) | 2 | Main trailer + one mobile unit traveling with the active work zone |
| Large commercial (75–200 workers) | 3–4 | Main trailer + active work-zone unit + one per major trade phase |
| High-rise (200+ workers, vertical site) | 4–8 | Ground trailer + one per 5–8 active floors + roof / man-lift staging |
| Heavy civil (highway, bridge, tunnel) | 2+ | Each work-zone trailer + traveling vehicle-mounted unit |
The trailer-vs-jobsite question
Most small construction sites have one centralized AED: in the foreman’s truck, the site office, or the supervisor’s tool crib. This works only if the entire active work zone is within 90-second round-trip retrieval.
Larger or vertical sites require mobile/portable AEDs that travel with the active trade. Best practice: assign one designated “AED carrier” per phase — typically the site safety officer or the lead trade foreman — who keeps the AED with them as the active work zone moves through the building.
Mobile/portable AED setup
- Lightweight unit (HeartSine 350P at 2.4 lb or Philips HeartStart FRx at 3.5 lb)
- High-visibility carry bag with reflective ISO 7010 signage
- Daily handoff log at shift start
- Status indicator check at every handoff
For drop-rated picks suited to active construction, see our best AED for construction sites guide.
High-rise construction: a special case
Vertical construction sites compound every challenge. Workers may be 30+ floors up, climbing temporary stairs, in zones with no elevator service yet. Standard AED placement breaks down completely.
The “every 5–8 active floors” rule
For high-rise construction, place an AED at every 5–8 active floors as the work progresses upward. Best practice:
- Ground trailer (always)
- One unit on every 5–8 actively worked floors
- Move AEDs up as floors complete and new floors activate
- Crane operators and tower-crane workers carry a personal AED-trained radio for rapid call response
Roof & man-lift staging
Roof workers and exterior man-lift crews face the longest EMS access times. Dedicated AED at roof staging plus radio communication with ground-floor first responders.
Real-world case
Hudson Yards (Manhattan) AED protocol
The Hudson Yards construction project — one of the largest in U.S. history — implemented a tiered AED program: ground-floor trailers (4), per-floor units on every 5th active floor, crane-deck units, and a dedicated safety vehicle with AED + first responder. Multiple cardiac events during construction were resolved successfully due to sub-3-minute device retrieval. Documented in industry safety reviews from 2014–2018.
Rugged cabinet & storage requirements
Construction-site AEDs face conditions that no office AED encounters:
- Dust & debris: Concrete, drywall, sawdust ingress — IP55+ minimum
- Temperature swings: -10°F winters and 110°F summers in many U.S. climates
- Theft risk: High-value equipment in unsecured zones — alarmed cabinet mandatory
- Drop/impact: Tools fall, scaffolding shifts — drop-tested AED preferred (Philips FRx, 1.5 m drop)
- Trailer relocation: Site offices move; AED mounting must be portable or quickly demountable
For high-vibration zones (near impact tools, demolition), use a transport bag rather than a wall-mount cabinet — vibration loosens mounting hardware over time.
Multi-trade coordination
A large jobsite involves a general contractor + multiple trade subcontractors (concrete, steel, electrical, mechanical, finishes). Coordinating AED responsibility:
- GC owns site-wide AED program — funds, installs, maintains
- Trade subs contribute training — at least 1 CPR/AED-certified worker per active trade per shift
- Document in site safety plan — AED locations, designated responders, EMS contact
- Pre-construction meeting — review AED placement with each new trade entering the site
The site safety plan should reference OSHA 1926.50 (Medical Services and First Aid) and include current AED placement diagrams updated weekly as work zones shift.
EMS pre-coordination
Construction sites often have access challenges that delay EMS response:
- The active site address may not yet appear in 911 databases
- Site entry gates may be locked or have changing access codes
- Multiple buildings under construction with no clear address
- Mud, debris, or temporary fencing blocking ambulance access
Pre-coordinate with local EMS at the start of every project: provide site address, GPS coordinates, gate access codes, and designated meeting point. Designate a worker at site entry during active hours to direct arriving EMS.
Subcontractor responsibility & insurance
Construction liability is layered. AED-related questions GCs should clarify in contracts:
- Does the GC’s general liability policy cover AED-related claims?
- Do trade subcontractor policies extend AED Good Samaritan protection?
- Are workers from temp agencies covered under the GC’s AED program?
- Who is responsible for maintenance: GC or trade sub?
Best practice: GC owns the AED program. Trade subs document their workers’ CPR/AED training and provide annual certifications. Workers’ compensation carriers often offer premium reductions for documented AED programs.
Tunnel, underground & confined-space sites
Underground construction (subway, utility tunnels, mining, sewer) creates unique challenges:
- Limited cellular reception → harder to call 911
- Longer evacuation routes → AED needs to be inside the work zone
- Atmospheric hazards (low O₂, gases) → secondary medical complications
- Confined space rescue protocols layer on top of the AED response
For these sites, the AED travels with the active work crew, paired with confined-space rescue equipment and pre-arranged surface response.
Who should buy/use this approach?
This framework fits:
- General contractors planning large-scale projects
- Site safety officers and certified safety professionals (CSPs)
- Trade subcontractors (concrete, steel, MEP, finishes)
- Project managers managing multi-month construction timelines
- Heavy civil contractors (highway, bridge, tunnel)
- Construction insurance brokers and risk managers
Frequently Asked Questions
Does OSHA require AEDs on construction sites?
Not specifically by regulation, but OSHA’s Best Practices Guide recommends them at any site with 50+ workers or where EMS response exceeds 5 minutes. The General Duty Clause creates de facto liability for foreseeable cardiac events without AED access.
How many AEDs does a large construction project need?
Roughly one per 75 active workers + one per major work zone. A high-rise project may require 4–8 units that move up as the building progresses. See our coverage table above for site-size guidance.
Should AEDs be in trailers or carried with workers?
Small sites (under 25 workers): trailer or site office is fine. Larger or vertical sites: combine fixed trailer units with mobile/portable AEDs that travel with the active work zone.
Who is responsible for the AED on a jobsite?
Best practice: the general contractor owns the program. Trade subcontractors contribute CPR/AED-trained workers and document certifications. Spell out responsibility in the master subcontract.
What AED is best for harsh construction conditions?
Drop-tested, IP-rated units like the Philips HeartStart FRx (1.5m drop, IP55) or HeartSine 450P (IP56). Pair with a steel-housed alarmed cabinet and store away from impact zones. See our construction AED guide for vetted picks.
Do AEDs work below freezing?
Most FDA-cleared AEDs operate at 32–122°F. Below 32°F, battery chemistry degrades, and the pad gel can freeze. For cold-climate winter construction, use a heated outdoor cabinet at fixed positions or keep the AED inside a heated trailer.
How do I pre-coordinate with EMS for a construction site?
Contact local EMS at project mobilization: provide site address, GPS coordinates, gate codes, designated meeting point, and key contact. Update if the site address or access changes. Designate a worker to direct EMS at the gate during active hours.
Sources & References
Disclaimer: Construction safety compliance is jurisdiction-specific. Consult your safety counsel and local OSHA Area Office. Insurance and contract requirements vary.